In survival analyses, higher plasma levels of COL3A1 propeptides were independently associated with better OS as well as DFS.
Collectively, these observations suggest that plasma COL3A1 propeptides may have greater utility for prognostic stratification than for diagnostic discrimination in OSCC.
Across multiple analytical approaches, higher plasma COL3A1 levels consistently emerged as a favourable prognostic factor.
Interestingly, CAF-D showed increased COL3A1 expression levels35, indicating that higher COL3A1 levels could exert antitumor effects.
In summary, plasma COL3A1 propeptides may serve as a prognostic biomarker in OSCC.
The current study focused on the most abundant non-cellular component in the TME, collagens, to better understand their role in predicting patients’ prognosis. By analysing plasma samples and tumour biopsies from OSCC patients, we investigated whether circulating collagen-derived peptides and their corresponding genes exhibit differential expression and possess prognostic value.
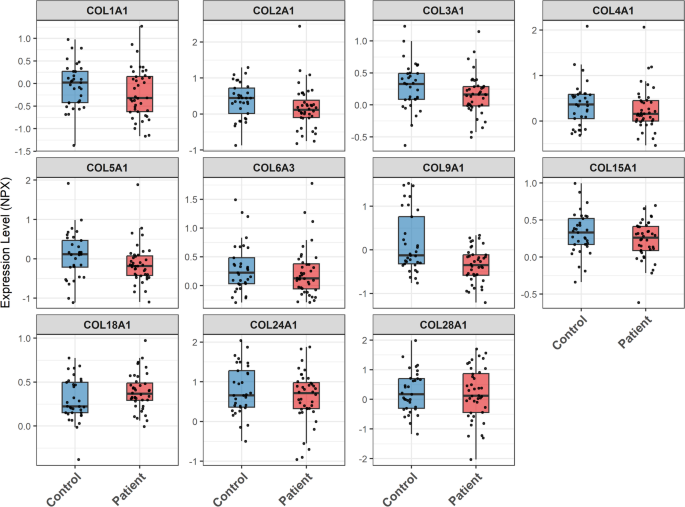
Our proteomic analysis identified 11 collagen-derived peptides in plasma, with similar levels observed in patients and healthy controls. At the mRNA level, eight corresponding collagen genes were upregulated in tumour tissue compared with both contralateral normal samples and healthy controls. Although the microarray cohort exhibited a substantial age difference between healthy controls (mean 40 years) and tumour patients (mean 61 years), the observed upregulation of collagen mRNA appears to be driven by tumour status rather than age, as clinically normal contralateral tissue (NTCT) did not differ significantly from healthy controls, whereas matched tumour versus NTCT comparisons within the same individuals showed clear differences.
Apart from significant correlations with age for several collagen peptides and significantly higher levels of COL24A1 peptides seen in smaller tumours (T1 + T2), the analysed collagens showed no correlations with sex or nodal status, either at the circulating peptide or local mRNA level. In survival analyses, higher plasma levels of COL3A1 propeptides were independently associated with better OS as well as DFS. Notably, COL3A1 mRNA was elevated in tumour tissues but was not independently associated with either OS or DFS.
COL3A1 is a fibrillar-forming collagen in the interstitial matrix and the second most abundant collagen in the body as well as a crucial component of the ECM. In peripheral blood, several studies of different solid tumours have demonstrated elevated levels of COL3A1 propeptides to be associated with poor prognosis19,27,28,29. In the measurement of COL3A1 in blood, different methods can be used. We applied measurement of the C- and N-terminus propeptides, which are released under active collagen formation30. An alternative is to measure so-called N-terminal telopeptides which are released during collagen degradation, as previously demonstrated by Nurmenniemi et al.31. In their study, by looking at the N-terminal telopeptide of COL3A1 in sera from patients with HNSCC high levels showed a connection to poor prognosis, even though not statistically significant. This result is in accordance with the present study where an association between high levels of C-terminal propeptides released during synthesis of COL3A1 and better OS and DFS was seen, whereas they saw an association between high levels of a marker for degradation of COL3A1 and poor prognosis31.
Comparing patients to controls, tumour tissue COL3A1 mRNA expression was elevated whereas circulating COL3A1 propeptides remained similar. Notably, the plasma cohort comprises multiple oral cavity subsites whereas the microarray tissue cohort is restricted to the oral tongue. Therefore, the tissue analyses provide complementary evidence of local ECM remodelling rather than a direct validation of the plasma results. Nevertheless, this discrepancy likely reflects the predominantly local nature of collagen deposition within the tumour microenvironment, as well as the fact that circulating collagen-derived peptides reflect overall extracellular matrix turnover rather than tumour-specific expression alone. In addition to tumour-associated remodelling, these markers may be influenced by non-malignant fibrotic or inflammatory processes in other tissues, while the presence of such conditions in the healthy controls was unknown. As procollagen propeptides are released into the circulation during collagen synthesis, contributions from multiple tissues may dilute tumour-derived signals in plasma32,33,34. Collectively, these observations suggest that plasma COL3A1 propeptides may have greater utility for prognostic stratification than for diagnostic discrimination in OSCC. Across multiple analytical approaches, higher plasma COL3A1 levels consistently emerged as a favourable prognostic factor. Univariate Kaplan-Meier analysis demonstrated improved survival for patients with high COL3A1, traditional multivariable Cox regression showed a protective effect after adjusting for clinical covariates, and LASSO-penalised Cox regression supported COL3A1 as a key predictor rather than a statistical artefact.
In OSCC, COL3A1 may, on the one hand, promote the formation of a dense extracellular matrix that physically restricts tumour cell migration and potentially contributes to improved patient survival. On the other hand, this matrix barrier could hinder the delivery of therapeutic agents and restrict immune infiltration at the tumour site. When co-transplanting CAFs, the main producers of COL3A1, with HNSCC cells into the mouse oral mucosa, distinct CAF behaviours were seen. CAF-P (promotor) surrounded cancer cells and promoted cancer cell invasion, whereas CAF-D (defence) formed a demarcated boundary and did not induce invasiveness. Interestingly, CAF-D showed increased COL3A1 expression levels35, indicating that higher COL3A1 levels could exert antitumor effects. Therefore, patients with high COL3A1 levels in tumour tissues may exhibit a paradoxical phenotype characterised by a more favourable baseline prognosis but potentially poorer responsiveness to certain systemic and immunological therapeutic approaches. This complexity is consistent with our finding that COL3A1 level in tumour tissue was not an independent predictor of survival.
In comparing plasma proteomic profiles between COL3A1-low and COL3A1-high patients, exploratory enrichment analysis of nominally differentially abundant proteins identified neutrophil degranulation as the most enriched pathway. This pathway included key neutrophil granule proteins, many of which were elevated in COL3A1-low patients. In line with prior evidence that tumour-associated neutrophils in OSCC contribute to extracellular matrix degradation, tumour invasiveness, and adverse clinical outcomes36, our findings raise the possibility that low circulating COL3A1 reflects a neutrophil-associated inflammatory state. Although direct evidence for neutrophil degranulation in HNSCC remains limited, accumulating data in OSCC/HNSCC support the involvement of neutrophil-related inflammatory programs in tumour progression, including associations with invasion, metastasis, and poor prognosis37,38,39. Proteomic evidence from early-stage gallbladder cancer further supports this biological link, as proteins related to neutrophil degranulation were identified alongside those involved in extracellular matrix remodelling40. Taken together, these findings suggest that elevated circulating COL3A1 levels are associated with a less inflammatory systemic profile, which mayreflect a more contained tumour microenvironment, whereas low COL3A1 levels may reflect a more neutrophil-driven and potentially more aggressive phenotype. This may partly account for the improved survival observed in patients with high COL3A1 levels. Notably, extracellular matrix remodelling in the tumour microenvironment is driven by multiple immune cell populations. Tumour-associated macrophages (TAMs), in particular, are recognised contributors to collagen turnover and matrix degradation through the secretion of matrix-remodelling enzymes and pro-fibrotic mediators41. The enrichment of immune system and innate immune system pathways further supports the involvement of a broader immune-stromal interaction network, particularly in the context of systemic inflammatory responses.
In summary, plasma COL3A1 propeptides may serve as a prognostic biomarker in OSCC. Of note, age was inversely correlated with plasma COL3A1 propeptide levels and is also an established determinant of overall survival, highlighting its potential role as a confounding factor. Although age was included as a covariate in the multivariable Cox model and COL3A1 remained independently associated with survival outcomes, the limited number of events restricts the robustness of this adjustment. Therefore, residual confounding cannot be fully excluded by statistical modelling alone. Consequently, the robustness and clinical applicability of these findings require validation in an independent cohort with an adequate number of events. Furthermore, larger paired tumour-plasma datasets will be necessary to clarify the relationship between tumour-derived ECM components and their representation in circulation. In addition, the lack of a significant difference in plasma COL3A1 levels between patients and healthy controls limits the interpretation of what constitutes a “high” value in a clinical setting. The establishment of clinically meaningful and absolute thresholds will be required.