
Human inflammatory bowel disease-on-a-chip for modelling disease progression, cancer initiation and sex-specific effects
This is not observed in the IBD or healthy epithelium in the absence of fibroblasts or in IBD epithelium with healthy fibroblasts. P = 0.0001 for H epithelium + H fibroblast versus IBD epithelium + IBD fibroblast, P = 0.0001 for H epithelium + H fibroblast versus H epithelium + IBD fibroblast, P = 0.001 for IBD epithelium + IBD fibroblast versus H epithelium + IBD fibroblast, P = 0.0004 for H epithelium + IBD fibroblast versus IBD epithelium + H fibroblast, P = 0.0003 for H epithelium + IBD fibroblast versus H epithelium without fibroblast, P = 0.0027 for H epithelium + IBD fibroblast versus IBD epithelium without fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus IBD epithelium + H fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus H epithelium without fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus IBD epithelium without fibroblast; n = 4 healthy, green; 2 CD, magenta; 2 UC, cyan. P = 0.0001 for H epithelium + H fibroblast versus IBD epithelium + IBD fibroblast, P = 0.0023 for H epithelium + H fibroblast versus H epithelium + IBD fibroblast, P = 0.0115 for H epithelium + IBD fibroblast versus IBD epithelium + H fibroblast, P = 0.0021 for H epithelium + IBD fibroblast versus H epithelium without fibroblast, P = 0.003 for H epithelium + IBD fibroblast versus IBD epithelium without fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus IBD epithelium + H fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus H epithelium without fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus IBD epithelium without fibroblast; n = 3 healthy, green; 1 CD, magenta; 2 UC, cyan. P = 0.0001 for H epithelium + H fibroblast versus IBD epithelium + IBD fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus H epithelium + IBD fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus IBD epithelium + H fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus H epithelium without fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus IBD epithelium without fibroblast, P = 0.0003 for H epithelium + IBD fibroblast versus H epithelium without fibroblast, P = 0.0215 for IBD epithelium + H fibroblast versus H epithelium without fibroblast, P = 0.0254 for H epithelium without fibroblast versus IBD epithelium without fibroblast; n = 3 healthy, green; 1 CD, magenta; 2 UC, cyan. For Basal graph: P = 0.0003 IBD epithelium + IBD fibroblast − strain versus H epithelium + H fibroblast + strain, P = 0.0015 IBD epithelium + IBD fibroblast − strain versus IBD epithelium + H fibroblast + strain, P = 0.0001 IBD epithelium + IBD fibroblast + strain versus IBD epithelium + H fibroblast + strain, P = 0.0001 IBD epithelium + IBD fibroblast + strain versus H epithelium + H fibroblast + strain, and for Apical graph: P = 0.0002 IBD epithelium + IBD fibroblast − strain versus H epithelium + H fibroblast + strain, P = 0.0003 IBD epithelium + IBD fibroblast − strain versus IBD epithelium + H fibroblast + strain, P = 0.0001 IBD epithelium + IBD fibroblast + strain versus IBD epithelium + IBD fibroblast − strain, P = 0.0001 IBD epithelium + IBD fibroblast + strain versus IBD epithelium + H fibroblast + strain, P = 0.0001 IBD epithelium + IBD fibroblast + strain versus H epithelium + H fibroblast + strain; n = 2 healthy, green; 2 CD, magenta; 2 UC, cyan.
Establishment of human healthy and IBD colon-on-a-chip devices
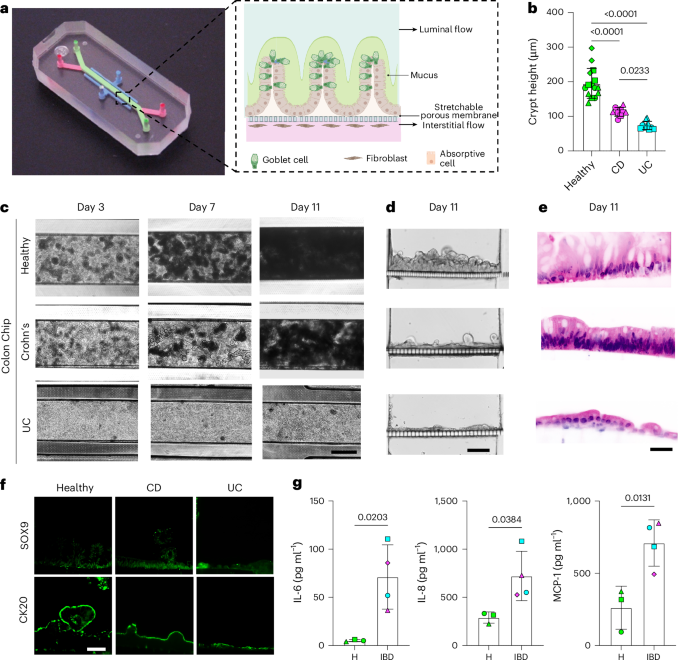
Patient-specific epithelial organoids and stromal fibroblasts were isolated from surgical resections of the colon of healthy donors and individuals with CD or UC (Supplementary Fig. 1a and Supplementary Information), and the organoids were expanded in Matrigel cultures, while the fibroblasts were cultured on plastic dishes (Supplementary Fig. 1b). To build the human colon-on-a-chip, primary colon epithelial cells and fibroblasts were respectively seeded on the top and bottom surfaces of a porous ECM-coated membrane that separates two parallel channels within a commercially available microfluidic organ-on-a-chip device (Fig. 1a). The cells were allowed to adhere under static conditions for 1 day before flow was initiated. A continuous epithelial monolayer with undulating crypt-like structures when viewed from above (Fig. 1b,c) or in cross sections (Fig. 1d,e) formed in healthy chips after 11 days. The epithelium became progressively obscured by dense opaque deposits from days 3 to 7, which completely filled the upper channel by day 11 (Fig. 1c). These opaque materials have been shown to be composed of mucus with similar composition, thickness and bilayer structure as seen in human colonic mucus in vivo12,13. Similar chips lined with colonic epithelium and fibroblasts from individuals with CD or UC also formed hills and crypt-like structures, but significantly less mucus accumulated on top of the epithelium, particularly in the UC chips (Fig. 1c and Supplementary Fig. 1c). Analysis of vertical cross-sectional views of the intestinal epithelium cultured in chips revealed that the heights of the undulating epithelial layer were significantly reduced in the IBD chips as well (Fig. 1d and Supplementary Fig. 1d). Epithelial cells within both healthy and IBD chips also expressed colon-specific cytokeratin 20 along their apical borders, while the basal stem cell marker SOX9 primarily appeared in their nuclei at the cell base (Fig. 1f), which is a hallmark of colon crypts in vivo15.
Fig. 1: Primary human colon-on-a-chip generated with epithelium and fibroblasts isolated from samples taken from healthy individuals and individuals with IBD. The alternative text for this image may have been generated using AI. Full size image a, Photograph of the commercially available organ-on-a-chip device (left) and a cross-sectional illustration of the epithelial–stromal tissue interface (right) formed with patient-derived cells, which is composed of a fibroblast-rich stroma that is perfused with medium to mimic interstitial fluid flow separated by a flexible, porous, ECM-coated membrane from a colon epithelium above. The epithelium, which is composed of absorptive cells and Goblet cells, secretes a thick mucus layer into the lumen of the apical channel that also experiences fluid flow. The entire tissue–tissue interface can be stretched and relaxed rhythmically to mimic peristalsis-like motions by applying cyclic suction to hollow side chambers in the flexible device (not shown). b, Height of crypts formed in colon-on-a-chip measured at 11 days. Numbers indicate P values between compared groups, as determined by one-way ANOVA test (P = 0.0001 for healthy versus CD; P = 0.0001 for healthy versus UC; P = 0.0233 for CD versus UC; n = 4 healthy, green; n = 3 CD, magenta; n = 3 UC, cyan). c, Representative brightfield microscopic images of healthy and IBD chips created with cells from individuals with CD or UC viewed from above on days 3, 7 and 11. A functional epithelial monolayer progressively accumulated mucus, which appears as opaque blackened fuzzy material, in the apical channel of all chips over the 11 day time course; however, mucus accumulation was suppressed in the IBD chips with the UC chips showing a greater reduction. Images that are shown are representative of replicates of 3 healthy individuals, 2 individuals with CD and 2 individuals with UC. Scale bar, 500 µm. d, Brightfield images of vertical cross-sections through healthy and IBD chips showing that the crypt-like epithelial structures are shorter in the CD and UC chips. Images that are shown are representative of replicates of 3 healthy individuals, 2 individuals with CD and 2 with UC. Scale bar, 100 µm. e, Histological haematoxylin-and-eosin-stained vertical cross-sections through healthy and IBD chips confirming the presence of columnar colon epithelium containing goblet cells in healthy epithelium, and a significant reduction in the height of the epithelial monolayer with reduced numbers of goblet cells in the IBD chips. Images that are shown are representative of replicates of 3 healthy individuals, 2 individuals with CD and 2 with UC. Scale bar, 50 µm. f, Immunofluorescence microscopic views showing distribution of SOX9 and CK20 in crypts in the colon epithelium of healthy and IBD chips. Images that are shown are representative of replicates of 3 healthy individuals, 2 individuals with CD and 2 with UC. Scale bar, 50 µm. g, Inflammatory cytokine protein levels measured in the basal outflows of healthy (H) and IBD chips on culture day 11 (chips were created with cells from 3 healthy donors (green), 2 individuals with CD (magenta) and 2 with UC (cyan), with each symbol representing a chip created with cells from a different patient. Numbers indicate P values between compared groups, as determined by two-tailed Student’s t-test. All data represent mean ± s.d.; P values are shown in all figures. Source data and statistical tests are provided. Diagram in a created in BioRender; Ozkan, A. https://biorender.com/f539sbd (2025). Source data
Previous work has shown that there is a subset of stromal fibroblasts in individuals with IBD that have higher levels of expression of oncostatin M receptor (OSMR) and podoplanin6, which appear to have an important role in inflammation, fibrosis and cancer16. Indeed, when we carried out flow cytometric analysis after removing stromal cells from the chips, we found that podoplanin expression was significantly higher in IBD fibroblasts that expressed high OSMR levels (Supplementary Fig. 2a,b) and that fibroblasts in IBD Chips lined by cells from individuals with CD or UC secreted more inflammatory cytokines (for example, IL6, IL8 and MCP-1 (also known as CCL2) from the basal channel than those in healthy chips (Fig. 1g). We also found that fibroblasts in IBD chips established using samples from individuals with CD or UC express higher vimentin and α-smooth muscle actin (α-SMA) than healthy controls (Supplementary Fig. 2c,d), as previously observed in IBD mice models induced by treatment with DSS or IL10 knock out17.
Transcriptomic analysis of epithelial cells and fibroblasts individually within Healthy versus IBD Chips revealed that genes which were found to be overexpressed in CD and UC (for example, ADA2, APOBEC3B, GSPT2, CD40, ACAN and HLA-DQB1) epithelium on-chip were also expressed at higher levels in the intestinal epithelium of individuals with IBD18,19,20,21,22 compared to healthy patients (Supplementary Fig. 3a,b). In addition, genes suppressed in tissues of individuals with IBD (for example, MUC5B and FDFT1 in CD and SOD3, SMIM32 and APOBR in UC18,19,20,21,22) were expressed at lower levels by epithelium in both CD and UC IBD Chips.
When stromal cells cultured in IBD chips were similarly analysed, they showed expression of IBD-relevant genes with CD fibroblasts overexpressing ITGA7, FXD1, HGF, FZD7, NKX2-3 and LOXL3 relative to healthy fibroblasts, while high levels of IKBIP, NKX2-3, ADA2, ECM2, NDN and SLC22A17 were seen in UC fibroblasts (Supplementary Fig. 3c,d). By contrast, other genes were downregulated in these fibroblasts including NLRP2, FUCA1, CLCA4 and RNF186 in CD and RALGPS1, DLG3, STON2 and FMO5 in UC-derived IBD chips (Supplementary Fig. 3c,d), which is again consistent with results of transcriptomic analyses carried out on tissues of individuals with IBD23,24,25.
Gene ontology and Reactome analysis revealed that multiple IBD-relevant biological processes, including increased ECM production and remodelling, cell adhesion and angiogenesis as well as decreased metabolism were predominant in both CD and UC epithelium and fibroblasts-on-chip, with UC tissues also showing suppressed IL10 signalling (Supplementary Fig. 4a–d). These functional pathways are also activated or suppressed in a similar manner in individuals with IBD26.
Peristalsis-like mechanical motions enhance IBD progression
Individuals with IBD experience thinning of the protective mucus layer in their colon12 and eventually loss of peristalsis as a consequence of increased fibrosis7,8, which further exacerbate their gastrointestinal symptoms. However, it is not known whether cyclic mechanical deformation of inflamed intestine or fluid flow due to peristalsis could influence IBD disease progression. To explore this possibility, we cultured healthy and IBD chips in the presence or absence of physiologically relevant cyclic deformations by applying suction to side chambers in the flexible devices. The healthy and IBD epithelia both accumulated a mucus layer when exposed to cyclic mechanical deformations, seen when viewed by darkfield imaging; however, the layer was much thinner in the IBD chips (Fig. 2a,b). Transcriptomic analysis confirmed that the IBD chips expressed lower levels of most mucins than healthy chips under all conditions, and that while expression of MUC1, MUC4, MUC12, MUC13, MUC17, MUC3A, MUC5AC and MUC5B increased in healthy chips exposed to mechanical strain, only MUC5AC and MUC13 increased in the IBD chips (Fig. 2c). These data show that peristalsis-like mechanical deformations have a direct effect on mucus production in the colonic epithelium in both healthy and IBD chips as fluid flow was constant under all conditions, and that the IBD epithelium is less effective at maintaining the normal thickness of the mucus layer in vitro as observed in individuals with IBD12,13.
Fig. 2: Peristalsis-like cyclic strain influences mucus production and fibrosis in the human colon-on-a-chip. The alternative text for this image may have been generated using AI. Full size image a, Representative side-view microscopy images of healthy or IBD chips with (+) and without (–) exposure to mechanical deformations visualizing mucus layer accumulation (white diffuse material) in healthy chips using darkfield microscopy. Note that limited mucus was produced by IBD epithelium. Scale bar, 1 mm. b, Quantification of the height of the mucus layer overlying healthy and IBD epithelium on-chip when cultured under the conditions in a. Numbers indicate P values between compared groups, as determined by one-way ANOVA test. P = 0.0003 for H− strain versus H+ strain; P = 0.0003 for H− strain versus IBD− strain; P = 0.0001 for H+ strain versus IBD− strain; P = 0.0001 for H+ strain versus IBD+ strain; P = 0.0013 for IBD− strain versus IBD+ strain; chips were created with cells from 3 healthy donors (green), 2 individuals with CD (magenta), and 2 with UC (cyan). c, Heat map of genes showing that peristalsis-like mechanical stimulation (+) increases expression of genes related to mucus production in healthy chips, but not IBD chips (n = 3 healthy, 2 CD and 2 UC). d, Second harmonic microscopic images of the fibroblast stroma in healthy versus IBD chips showing greater collagen fibril accumulation (green) with mechanical strain (+Strain) in both chips and that this response is greatly accentuated in IBD chips. Scale bar, 200 μm. e, Collagen fibril signal intensity in the stroma of healthy versus IBD chips quantified in second harmonic generated (SHG) microscopic images. a.u., arbitrary units. Numbers indicate P values between compared groups, as determined by one-way ANOVA test (P = 0.0001 for H− strain versus IBD+ strain; P = 0.0001 for H+ strain versus IBD+ strain; P = 0.0001 for IBD− strain versus IBD+ strain; chips were created with cells from 3 healthy donors (green), 2 individuals with CD (magenta) and 2 with UC (cyan). f, Heat map of genes showing that peristalsis-like cyclic strain enhances expression of genes associated with fibrillar collagen production in IBD fibroblasts, but not in healthy fibroblasts (n = 3 healthy, 2 CD and 2 UC). g, Heat maps showing that cyclic strain enhances greater expression of IBD-associated inflammatory genes in IBD chips compared to healthy chips in both epithelium and fibroblasts (n = 3 healthy, 2 CD and 2 UC). Source data and statistical tests are provided. Source data
Second harmonic imaging of ECM fibre formation on-chip revealed that while both CD- and UC-derived IBD fibroblasts accumulate comparable fibrillar collagen as healthy cells, these levels increase many fold when the IBD chips are exposed to peristalsis-like motions, whereas there is no change in healthy chips (Fig. 2d,e). Atomic force microscopic analysis carried out in parallel samples from the resections we used to isolate the patient-derived cells confirmed that this was associated with tissue stiffening (Supplementary Fig. 5a–d). But while transcriptomic analysis showed that there is increased expression of collagen-associated genes in CD and UC stroma on-chip without mechanical strain, exposure to peristalsis-like deformations did not result in significant changes in collagen gene expression (Fig. 2f), suggesting that the fibrotic changes we observed resulted from post-transcriptional alterations. Indeed, pathway analysis confirmed that biological processes associated with fibrosis per se (ECM organization, collagen formation and fibril organization) were upregulated in IBD chips upon exposure to cyclic mechanical deformations (Supplementary Fig. 6a). In addition, our transcriptomic analysis revealed that expression of different cytochrome P450 subunits was suppressed in IBD versus healthy chips, which is consistent with the observation that the intestinal tissues of individuals with IBD experience decreased metabolic activities27,28. While peristalsis-like cyclic deformations increased the expression of most of these metabolic genes in healthy chips, this response was not observed in IBD chips (Supplementary Fig. 6b).
Peristalsis-like cyclic deformations also increased barrier permeability in both healthy and IBD chips; however, barrier leakiness always remained higher in IBD Chips (Supplementary Fig. 7a). Mechanical stimulation also enriched expression of inflammation-associated genes in epithelial cells and fibroblasts in both healthy and IBD chips (Fig. 2g), and this was supported by transcriptomic analysis, which showed activation of the inflammatory response pathway in these cells (Supplementary Fig. 7b). Further pathway analysis of this transcriptomic dataset (Supplementary Fig. 8) showed that peristalsis-like deformations activate pathways associated with IBD progression and exacerbation in the epithelium, including those involved in cancer, Toll-like receptor signalling, PPAR signalling, and focal adhesion in IBD epithelium (Supplementary Fig. 9a) as well as NOD-like receptor signalling, PDGF signalling and cytokine–cytokine receptor interaction in IBD fibroblasts (Supplementary Fig. 9b). By contrast, these pathways that are known to exacerbate colitis in individuals with IBD29,30 were not activated in healthy chips under the same mechanical stimulation conditions.
Replicating sex-specific clinical symptoms of individuals with IBD
The gastrointestinal symptoms of female individuals with IBD become much more prominent during menstrual periods2, and their therapies need to be optimized to control their symptoms before pregnancy because of increased risk of miscarriage, preterm birth and low birth weight3. Yet, it is not known whether these responses are a direct effect of ovarian hormones on the intestine, which could potentially contribute to the clinical observations observed in patients31. To address this question directly, we exposed healthy and IBD chips lined by cells from female patients to oestrogen (E2) and medroxyprogesterone acetate (MPA) to recapitulate the menstrual cycle or a mixture of pregnancy-associated hormones (E2, MPA, human chorionic gonadotropin, prolactin and placental lactogen) to mimic the first trimester of pregnancy. Exposure to E2 and MPA or the pregnancy-associated hormone mixture increased the height of crypt-like epithelial structures in both healthy and IBD chips (Fig. 3a–c). We also discovered addition of E2 and MPA increased fibrosis, and exposure to the pregnancy-associated hormone mixture produced an even greater increase in fibrillar collagen deposition in the stroma of IBD chips; however, this was not observed in healthy chips (Fig. 3d,e and Supplementary Fig. 10). Exposure to E2, MPA or the pregnancy-associated hormone mixture decreased overall inflammatory cytokine and chemokine production in healthy chips, whereas levels of these inflammatory molecules increased when IBD chips were exposed to the same hormones (Fig. 3f).
Fig. 3: Effects of ovarian hormones in female colon chips. The alternative text for this image may have been generated using AI. Full size image a,b, Differential interference contrast microscopic images from above (a) and vertical cross-sectional views of confocal microscopic images (b) of healthy and IBD chips 7 days after treatment with exposure to E2, E2 plus MPA, or PAH. PAH, pregnancy-associated hormone. a, When viewed from above, exposure to PAH appeared to slightly increase the density of crypt-like structures in both healthy and IBD chips. Scale bar, 500 µm. b, When viewed in vertical cross-sections, the number and height of crypt-like structures increased when exposed to PAH as well as E2 + MPA in both healthy and IBD chips, although the scale of the response was much less in the IBD chips. Scale bar, 100 µm. Magenta, phalloidin; cyan, DAPI; dashed white line, upper surface of chip membrane; dashed yellow line, upper luminal boundary of the crypt. c, Quantification of heights of crypt-like structures in healthy and IBD chips in the presence or absence of different combinations of the ovarian hormones (E2, MPA and PAH), as indicated. Numbers indicate P values between compared groups, as determined by one-way ANOVA test; healthy chips graph: P = 0.0026 for −E2 −MPA −PAH versus +E2 +MPA −PAH; P = 0.0001 for −E2 −MPA −PAH, versus +E2 +MPA +PAH; IBD: P = 0.0001 −E2 −MPA −PAH versus +E2 +MPA −PAH; P = 0.0001 for −E2 −MPA −PAH versus +E2 +MPA +PAH; chips were created with cells from 2 healthy donors (green), 1 individual with CD (magenta) and 2 with UC (cyan). d, Second harmonic microscopic images of fibrillar collagen (green) produced by fibroblasts in response to the different hormonal conditions shown in a and b showing a much greater fibrosis response in the IBD chips compared to healthy when exposed to a pregnancy-mimicking hormone combination (E2 + MPA + PAH). Scale bar, 200 μm. e, Graphs showing quantification of collagen fibril signal intensity in the stroma of healthy versus IBD chips using second harmonic microscopic imaging. Numbers indicate P values between compared groups, as determined by one-way ANOVA test. P = 0.0023 for −E2 −MPA −PAH versus +E2 +MPA +PAH; P = 0.0010 for +E2 −MPA −PAH versus +E2 +MPA +PAH; P = 0.0080 for +E2 +MPA −PAH versus +E2 +MPA +PAH; chips were created with cells from 2 healthy donors (green), 1 individual with CD (magenta) and 2 with UC (cyan). f, Heat maps showing production of pro-inflammatory cytokine and chemokine proteins in apical (epithelial) and basal (fibroblast) channels of healthy versus IBD chips 7 days after treatment with different female hormone exposures, as indicated. P values were determined by one-way ANOVA test. *P < 0.05. Note that exposure to female hormones significantly increased expression of inflammatory factors in both the epithelium and fibroblasts in IBD chips, whereas they suppressed their production in healthy chips (chips were created with cells from 2 healthy donors (green), 1 individual with CD (magenta) and 2 with UC (cyan). Source data and statistical tests are provided; P values are shown in all figures. Source data
Stromal fibroblasts control barrier permeability and epithelial inflammation
To better understand the role of fibroblasts in IBD, we took advantage of the synthetic biology nature of human organ-on-a-chip technology to create chips lined by heterotypic tissue recombinants of healthy epithelium with IBD stroma and vice versa. As expected, the homotypic cultures of IBD epithelium and stroma had a compromised barrier with higher permeability than healthy epithelium and stroma recombinants (Fig. 4a). However, we discovered that the presence of the IBD fibroblasts was the key driver of barrier disruption as permeability increased significantly when they were combined with healthy epithelium in tissue recombinant chips, even though there was no difference in permeability when the different epithelia were cultured alone (Fig. 4a). The permeability of the IBD epithelium alone (that is, without IBD stroma) was similar to that of healthy epithelium with or without healthy fibroblasts, and tissue recombinants combining healthy fibroblasts with IBD epithelium also did not further alter barrier function, again emphasizing the key role that the IBD stroma has in terms of compromising intestinal barrier function.
Fig. 4: Tissue recombinant chips reveal that the IBD fibroblasts drive compromise of the permeability barrier and inflammation in the epithelium. The alternative text for this image may have been generated using AI. Full size image a, Graph showing that intestinal barrier permeability to cascade blue is much higher in homotypic IBD chips compared to healthy chips and that tissue recombinants of IBD fibroblasts with healthy epithelium results in a similar high level of barrier compromise on-chip. This is not observed in the IBD or healthy epithelium in the absence of fibroblasts or in IBD epithelium with healthy fibroblasts. Numbers indicate P values between compared groups, as determined by two-way ANOVA with post hoc Tukey’s multiple-comparison test. P = 0.0001 for H epithelium + H fibroblast versus IBD epithelium + IBD fibroblast, P = 0.0001 for H epithelium + H fibroblast versus H epithelium + IBD fibroblast, P = 0.001 for IBD epithelium + IBD fibroblast versus H epithelium + IBD fibroblast, P = 0.0004 for H epithelium + IBD fibroblast versus IBD epithelium + H fibroblast, P = 0.0003 for H epithelium + IBD fibroblast versus H epithelium without fibroblast, P = 0.0027 for H epithelium + IBD fibroblast versus IBD epithelium without fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus IBD epithelium + H fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus H epithelium without fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus IBD epithelium without fibroblast; n = 4 healthy, green; 2 CD, magenta; 2 UC, cyan. b, Quantification of cytokine protein levels revealed that combinations of IBD fibroblasts with healthy epithelium result in increased production of IL-6 and MCP-1 in the colon-on-a-chip, whereas this was not seen in healthy epithelium alone or homotypic chips. Numbers indicate P values between compared groups, as determined by one-way ANOVA with post hoc Tukey’s multiple-comparison test. P = 0.0001 for H epithelium + H fibroblast versus IBD epithelium + IBD fibroblast, P = 0.0023 for H epithelium + H fibroblast versus H epithelium + IBD fibroblast, P = 0.0115 for H epithelium + IBD fibroblast versus IBD epithelium + H fibroblast, P = 0.0021 for H epithelium + IBD fibroblast versus H epithelium without fibroblast, P = 0.003 for H epithelium + IBD fibroblast versus IBD epithelium without fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus IBD epithelium + H fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus H epithelium without fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus IBD epithelium without fibroblast; n = 3 healthy, green; 1 CD, magenta; 2 UC, cyan. c, IL-6 and MCP-1 production by IBD epithelium also required the presence of IBD fibroblasts. Numbers indicate P values between compared groups, as determined by one-way ANOVA with post hoc Tukey’s multiple-comparison test. P = 0.0001 for H epithelium + H fibroblast versus IBD epithelium + IBD fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus H epithelium + IBD fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus IBD epithelium + H fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus H epithelium without fibroblast, P = 0.0001 for IBD epithelium + IBD fibroblast versus IBD epithelium without fibroblast, P = 0.0003 for H epithelium + IBD fibroblast versus H epithelium without fibroblast, P = 0.0215 for IBD epithelium + H fibroblast versus H epithelium without fibroblast, P = 0.0254 for H epithelium without fibroblast versus IBD epithelium without fibroblast; n = 3 healthy, green; 1 CD, magenta; 2 UC, cyan. d, Peristalsis-like cyclic strain preferentially stimulates migration of PBMCs (magenta) from the fibroblast stroma in the basal channel (Basal) to the epithelium in the apical channel (Apical) in IBD chips but not in heterotypic chips with IBD epithelium and healthy fibroblasts or in healthy chips. e, Quantification of the results from d confirmed that IBD chips showed higher baseline recruitment of PBMCs to the surface of the fibroblast stroma in the basal channel and that this was not altered by mechanical strain, whereas IBD epithelium combined with healthy stroma or healthy chips only showed significantly less PBMC recruitment. By contrast, the number of PBMCs that migrated to the epithelium in the apical channel more than doubled in IBD chips when they were exposed to peristalsis-like mechanical deformations, and overall migration of PBMCs was minimal when IBD fibroblasts were absent. Numbers indicate P values between compared groups, as determined by one-way ANOVA test. For Basal graph: P = 0.0003 IBD epithelium + IBD fibroblast − strain versus H epithelium + H fibroblast + strain, P = 0.0015 IBD epithelium + IBD fibroblast − strain versus IBD epithelium + H fibroblast + strain, P = 0.0001 IBD epithelium + IBD fibroblast + strain versus IBD epithelium + H fibroblast + strain, P = 0.0001 IBD epithelium + IBD fibroblast + strain versus H epithelium + H fibroblast + strain, and for Apical graph: P = 0.0002 IBD epithelium + IBD fibroblast − strain versus H epithelium + H fibroblast + strain, P = 0.0003 IBD epithelium + IBD fibroblast − strain versus IBD epithelium + H fibroblast + strain, P = 0.0001 IBD epithelium + IBD fibroblast + strain versus IBD epithelium + IBD fibroblast − strain, P = 0.0001 IBD epithelium + IBD fibroblast + strain versus IBD epithelium + H fibroblast + strain, P = 0.0001 IBD epithelium + IBD fibroblast + strain versus H epithelium + H fibroblast + strain; n = 2 healthy, green; 2 CD, magenta; 2 UC, cyan. Source data and statistical tests are provided. Source data
This controlling effect of IBD fibroblasts on barrier function when combined with healthy epithelium was also accompanied by increased production of multiple inflammatory cytokines and chemokines including IL-6, MCP-1 (Fig. 4b,c), IL-8 (also known as CXCL8), CXCL-1, LIF, IL-21, PIGF-1 and MIP-1β (also known as CCL4) (Supplementary Fig. 11a) relative to chips lined by healthy fibroblasts and epithelium or healthy epithelium alone. However, the IBD epithelium appeared to constitutively express high levels of all these cytokines regardless of whether or not IBD fibroblasts were present or they were replaced with healthy fibroblasts, except for production of IL-6 and MCP-1 that were further enhanced by the presence of the IBD stroma (Fig. 4b,c and Supplementary Fig. 11b). As these two cytokines are known to promote monocyte infiltration into stroma from the vascular system and their differentiation to macrophage cells32, we perfused human peripheral blood mononuclear cells (PBMCs) through the basal channel of the colon-on-a-chip. We found that more PBMCs adhered to the stroma and migrated to the epithelial channel in the IBD chips compared to healthy chips (Fig. 4d). While application of peristalsis-like deformations did not alter PBMC adhesion to the stroma in the basal channel, it significantly enhanced the migration of these cells to the epithelium in the apical channel, but only in IBD chips (Fig. 4e). However, when we carried out a similar study in a heterotypic tissue recombinant chip containing IBD epithelium with healthy fibroblasts, PBMC recruitment and migration were suppressed and reverted to the low levels observed in healthy chips (Fig. 4d,e). This finding correlates well with transcriptomic analysis, which revealed that multiple surface receptors for immune cell adhesion are expressed at higher levels in fibroblasts and epithelium in IBD chips versus healthy chips (Supplementary Fig. 11c). IBD chips co-cultured with PBMCs also showed increased production of IL-6 and IL-8 in both their apical and basal channels, whereas this was not observed with healthy chips (Supplementary Fig. 11d).
Modelling early cancer progression in human IBD chips
Individuals with IBD have a higher incidence of CRC formation33, and this also has been demonstrated in animal IBD models by exposing them to the carcinogen N-ethyl-N-nitrosourea (ENU)34. When we exposed healthy and IBD chips created with cells from multiple different donors to ENU (10 μg ml−1) for 3 weeks, we observed a decrease in the height of crypt-like structures (Fig. 5a,b) and an increase in barrier permeability (Fig. 5c) in both in healthy and IBD chips. However, ENU had a much greater impact on inflammatory cytokine secretion in the IBD chips (Fig. 5d), and it resulted in a greater reduction of E-cadherin expression in IBD chips versus healthy chips, which was accompanied by a concomitant increase in β-catenin translocation to the nucleus (Fig. 5e,f). Similar activation of the β-catenin signalling pathway has previously been shown to be associated with CRC progression35. In addition, ENU treatment promoted enlargement of epithelial nuclei and a decrease in their roundness, which are also known to accompany early carcinogenesis36. Shallow pass genome sequencing revealed increased gene mutations and duplication in IBD chips but not in healthy chips (Fig. 5g). The CD chips showed a higher level of gene amplification (indicated by green bars in Fig. 5g) than chips lined with cells from individuals with UC, and an existing mutation in one individual with CD was further amplified after ENU exposure.
Fig. 5: Exposure to carcinogen preferentially promotes mutagenesis and early steps in carcinogenesis in IBD chips. The alternative text for this image may have been generated using AI. Full size image a, Differential interference contrast microscopic images of the epithelium when viewed from above in healthy and IBD chips after 21 days of culture in the presence or absence of the carcinogen (ENU) showing that undulating crypt-like structures are lost in both healthy and IBD chips after exposure to ENU. Scale bar, 500 µm. b, Quantification of results from a showing that ENU decreases height of the epithelium in both healthy and IBD chips. Numbers indicate P values between compared groups, as determined by one-way ANOVA with post hoc Tukey’s multiple-comparison test. P = 0.0001 for H – ENU versus H + ENU; P = 0.0001 for H − ENU versus IBD − ENU; P = 0.0001 for H − ENU versus IBD + ENU; P = 0.0014 for IBD − ENU versus IBD + ENU; n = 3 healthy, green; 2 CD, magenta; 2 UC, cyan. c, Epithelial barrier permeability increased as a result of exposure to ENU in healthy and IBD chips. Numbers indicate P values between compared groups, as determined by one-way ANOVA test. P = 0.0001 for H − ENU versus IBD + ENU; P = 0.0104 for H − ENU versus H + ENU; P = 0.0307 for H − ENU versus IBD − ENU; P = 0.0476 for H + ENU versus IBD + ENU; P = 0.0075 for IBD − ENU versus IBD + ENU; n = 4 healthy, green; 2 CD, magenta; 2 UC, cyan. d, Heat map showing inflammatory cytokine protein levels measured in outflows from the apical channel of healthy and IBD chips 3 weeks after ENU exposure. ENU exposure significantly increased inflammatory cytokine production in IBD chips made with cells from both CD and UC tissue donors compared to healthy patients. e, Confocal microscopic top-view images showing β-catenin and E-cadherin localization and nuclear staining (DAPI) in the epithelium within healthy and IBD chips 3 weeks after ENU exposure. Scale bar, 20 μm. f, Quantification of protein staining intensity and morphology reveal that ENU exposure decreases E-cadherin (P = 0.0023) levels and increases nuclear localization of β-catenin (P = 0.0001) in chips derived from individuals with IBD compared to healthy chips. ENU exposure also resulted in greater nucleus size (P = 0.0188) and less roundness (P = 0.0003). Numbers indicate P values between compared groups, as determined by two-tailed Student’s t-test (n = 3 healthy, green; 2 CD, magenta; 2 UC, cyan). g, Plots showing copy number changes across all human chromosomes in healthy and IBD chips before (red) and 3 weeks after ENU exposure (blue). Green bars indicate amplification of gene sequences for the whole chromosome. Each graph represents an individual healthy chip or chip derived from an individual with IBD. h, Confocal microscopic top-view images showing early-stage CRC marker, CEACAM5, expression in healthy and IBD epithelium when they are cultured with or without healthy fibroblasts or IBD fibroblasts and exposed to ENU for 3 weeks. Source data and statistical tests are provided. Source data
We then investigated whether the fibroblast phenotype influences the propensity for cancer formation following ENU exposure in healthy versus IBD epithelium cultured on-chip. CEACAM5 is an early-stage CRC marker37, which is expressed only in CRC tissues and not in healthy and IBD intestinal epithelium in vivo (Supplementary Fig. 12a). When we analysed its expression in epithelium in our heterotypic and homotypic tissue recombinants on-chip, we found that neither healthy nor IBD epithelium expressed CEACAM5 on-chip under baseline conditions without ENU exposure (Supplementary Fig. 12b). Healthy epithelium exposed to ENU expressed CECAM5 but only when cultured with IBD fibroblasts (Fig. 5h and Supplementary Fig. 12c). The presence of IBD fibroblasts also enhanced expression of CEACAM5 in IBD epithelium when exposed to ENU, although lower levels of CEACAM5 expression were observed even when IBD epithelium was cultured alone or with healthy fibroblasts. A greater reduction in E-cadherin expression (Supplementary Fig. 12d,e), along with β-catenin translocation to the nucleus, were also seen in IBD epithelium cultured with IBD fibroblasts when exposed to ENU (Supplementary Fig. 12f). Taken together, these data show that IBD fibroblasts have an important role in driving an increased propensity for cancer initiation in intestinal epithelium.





© All Rights Reserved.